Quick Summary:
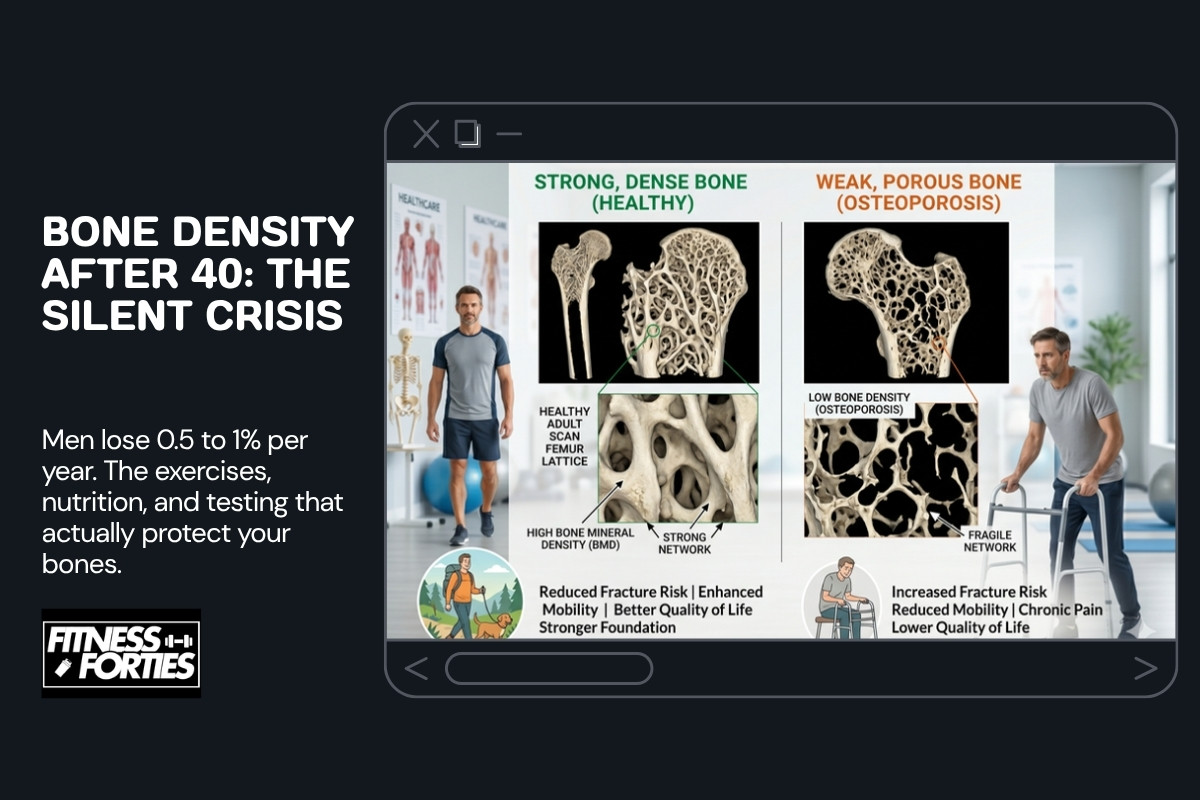
- Men over 40 lose 0.5 to 1% of bone density per year, yet fewer than 5% get tested before their first fracture.
- Weight-bearing exercises like heavy squats and deadlifts can increase bone mineral density by 1 to 3% annually when combined with adequate vitamin D (2,000 to 4,000 IU) and protein (1.6 to 2.2g/kg).
- A baseline DEXA scan at 40 costs $50 to $200 and gives you the data to track and reverse bone loss before it becomes irreversible.
Table of contents
- Why men ignore bone density until it’s too late
- How bone density changes after 40 in men
- The 5 biggest risk factors for bone density loss in men over 40
- How to test and track your bone density
- The best exercises for bone density for men over 40
- Nutrition and supplements that actually support bone health
- Why bone density is a household conversation
- Frequently asked questions
- Final thoughts
Introduction
Bone density for men over 40 is one of the most overlooked health metrics. We worry about muscle loss, belly fat, declining testosterone. We track those metrics obsessively. But bones? They’re silent. You don’t feel them thinning 0.5% per year until something cracks.
During my body transformation at 42 with coach Charlie Johnson at CJ Fitness, I was focused on body composition: tracking protein, measuring lifts, managing calories. Bone density wasn’t on my radar at all. It was only when I started researching deeper into longevity and health optimization that I realized bones are the silent foundation everything else depends on. You can be strong, lean, and metabolically healthy on the surface while your skeleton quietly becomes brittle underneath. Now getting a DEXA scan is on my to-do list, and I want to share what I’ve learned about why it matters and what actually works.
Here’s the sobering part: fewer than 5% of men over 40 get screened before their first fracture. The International Osteoporosis Foundation reports that a 50-year-old man has a 1 in 5 chance of an osteoporotic fracture in his remaining lifetime. A hip fracture at 65 isn’t just a broken bone: it’s a 20% increased risk of death within the first year, often from complications like blood clots or pneumonia. Think of bone density like tracking an asset losing value. You wouldn’t ignore a portfolio bleeding 0.5% annually without understanding why. Yet that’s exactly what most men do with their skeletons.

Why men ignore bone density until it’s too late
The International Osteoporosis Foundation found that osteoporosis is responsible for more days spent in hospital than many other chronic diseases, including heart attacks, prostate cancer, and diabetes combined. A hip fracture at 70 often means the end of independence. You either recover in a nursing home or you don’t recover at all.
Yet most men have never heard the word “T-score” and don’t know what a DEXA scan is. Why? Because osteoporosis is marketed as a woman’s disease. It’s not. Men just develop it later, typically after 70, which means many assume they’re safe until then. That’s the trap. By the time symptoms show up, you’ve already lost 30 to 40% of your bone mineral density. You don’t get it back with a pill.
The second reason men ignore it: bone density is invisible. Muscle loss is visible. A belly is visible. Low testosterone shows up in blood work and your mood. But bone density? You need a specialized scan to know the truth. Most men go their entire lives without ever getting that scan.
How bone density changes after 40 in men
Your bones aren’t static. They’re living tissue constantly breaking down and rebuilding. Two types of cells do this work: osteoclasts (which break down bone) and osteoblasts (which build new bone). In your 20s and 30s, osteoblasts outpace osteoclasts. You’re building bone faster than you’re losing it. Peak bone mass happens around age 30, then stays relatively flat until about age 40.
After 40, osteoclasts start winning the race. Bone breakdown accelerates while bone formation slows. Men lose approximately 0.5 to 1% of bone density per year after age 40, accelerating slightly after age 70. Over 30 years, that’s 15 to 30% loss. A small amount is normal aging. But most men lose far more than biology demands because they’re sedentary, vitamin D deficient, or eating insufficient protein.
The good news: this decline is not inevitable. You can slow it, stop it, and even reverse years of loss with the right stimulus and nutrition. The bad news: you have to be intentional about it. Your genetics set the baseline, but your behavior determines whether you keep what you have.
The 5 biggest risk factors for bone density loss in men over 40
1. Sedentary lifestyle
Bones adapt to load. No load, no adaptation. A man sitting in an office 8 hours a day, commuting by car, and watching TV in the evening is sending his skeleton a signal: you’re not needed. Osteoclasts listen to that signal and accelerate bone breakdown.
Conversely, a man doing heavy squats, deadlifts, and loaded carries is sending the opposite signal: you’re critical. Osteoblasts respond by building bone. This is called mechanotransduction: your bones literally sense mechanical stress and adapt to it. No stress, no adaptation.
2. Low testosterone
Testosterone is anabolic for bone. It stimulates osteoblasts and increases calcium absorption in the gut. Men with low testosterone (below 300 ng/dL) have accelerated bone loss. This is why some men on suppressive cancer treatments or with hypogonadism develop osteoporosis in their 50s rather than their 70s.
If you suspect low testosterone, get tested. But don’t assume TRT is the answer. Strength training increases testosterone naturally and also directly stimulates bone formation regardless of hormone levels.
3. Vitamin D deficiency
Vitamin D controls calcium absorption. Without adequate vitamin D, your gut cannot absorb dietary calcium efficiently. Your body compensates by pulling calcium from your bones, weakening them in the process. Men in northern latitudes or those who spend most of their time indoors are at high risk.
I live in Switzerland, at 47 degrees north latitude. From November to March, the sun angle is too low for skin synthesis of vitamin D. Sunscreen, even when needed for sun protection, further reduces vitamin D synthesis. Most Swiss men are vitamin D deficient in winter without supplementation.
Optimal 25-hydroxyvitamin D levels for bone health are 30 to 50 ng/mL (75 to 125 nmol/L). Most men need 2,000 to 4,000 IU daily to maintain this range, more if you live north of 40 degrees latitude or have darker skin.
4. Excessive alcohol consumption
Alcohol is toxic to osteoblasts. Heavy drinking (more than 3 drinks per day) directly suppresses bone formation. Additionally, alcohol impairs vitamin D metabolism and increases calcium loss through the kidneys. Heavy drinkers have 2 to 3 times higher fracture risk regardless of bone density.
Moderate drinking (1 to 2 drinks per day) appears safe for bone health. Beyond that, you’re trading short-term pleasure for long-term skeletal integrity.
5. Chronic cardio without resistance training
Long-distance running, cycling, and swimming have minimal skeletal loading. A man doing 5 hours of cycling per week but no resistance training will have poor bone density despite being aerobically fit. These activities are valuable for heart health and metabolic health, but they don’t stimulate bone formation.
The research is clear: resistance training with heavy loads is the primary driver of bone density. Aerobic exercise is complementary but not sufficient on its own. I cover this in detail in the exercise section below. If you’re interested in building aerobic capacity while loading your skeleton, rucking combines zone 2 cardio with skeletal loading.
A note on GLP-1 medications and bone density
If you’re taking semaglutide (Ozempic, Wegovy) or another GLP-1 receptor agonist for weight loss, bone density deserves extra attention. A 2025 study published in the Journal of Bone and Mineral Research found that GLP-1 users had approximately 30% higher risk of osteoporosis compared to non-users. Rapid weight loss from these medications can reduce bone mineral density by 1.6 to 2.8% within 12 months, particularly at the hip and spine.
The mechanism is straightforward: when you lose weight rapidly, you lose both fat and lean mass. Less mechanical load on your skeleton means less stimulus for osteoblasts. Combined with the caloric deficit these drugs create, your body may pull calcium from bones to maintain blood levels. This is not a reason to avoid GLP-1 medications if they’re medically appropriate. It is a reason to pair them with resistance training and ensure adequate calcium, vitamin D, and protein intake. If you’re on a GLP-1 drug and over 40, a baseline DEXA scan before starting treatment gives you real data to monitor.
How to test and track your bone density
The gold standard test for bone density is a DEXA scan (dual-energy X-ray absorptiometry). It’s a simple, non-invasive 10-minute scan that measures bone mineral density at your spine, hip, and forearm. The radiation dose is negligible (about 1/10 of a chest X-ray). DEXA results are reported as T-scores and Z-scores.
A T-score compares your bone density to a healthy 30-year-old of the same sex. Z-scores compare you to age-matched peers. The scoring system: T-score above minus 1.0 is normal, minus 1.0 to minus 2.5 is osteopenia (low bone mass), below minus 2.5 is osteoporosis. For men, T-scores are typically more relevant than for women because we don’t have a specific age-related decline cutoff like menopause.
DEXA scan costs range from $50 to $200 depending on location and provider. In Switzerland, DEXA is covered by mandatory health insurance if you have risk factors (age over 70, previous fracture, long-term corticosteroid use, or medical conditions affecting bone health). Otherwise, it’s out of pocket, typically CHF 150 to 300.
I’ll be honest: I haven’t had a DEXA scan yet. Writing this article moved it to the top of my priority list. When I ran blood work through Care in Zurich earlier this year, bone density wasn’t part of the panel. That’s the problem with this topic: it doesn’t show up in standard blood tests. You need to specifically request a DEXA scan.
If you’re in Switzerland and want to start with blood work as a baseline health check, I use Care for convenient lab testing. But for bone density specifically, you’ll need to ask your doctor for a DEXA referral.
Once you have a baseline, repeat the scan every 2 years if you’re normal, annually if you’re in the osteopenia range. This gives you concrete data to track whether your training and nutrition are actually working. Tracking bone density for men over 40 means you stop guessing and start measuring. Instead of hoping things are improving, you have proof.
The best exercises for bone density for men over 40
The key to improving bone density for men over 40 comes down to one principle: bones adapt to mechanical load through a process called mechanotransduction. When osteocytes (cells embedded in bone matrix) sense stress, they signal osteoblasts to build more bone. The stimulus must be high-force and novel. Repeating the same easy movement doesn’t trigger adaptation. You need heavy loads, explosive movements, or impact.
The exercise ranking for bone density, from highest to lowest impact:
- Heavy resistance training (squats, deadlifts, loaded carries): High impact. Loading your spine and lower body with heavy weights is the single most effective stimulus for bone density.
- Plyometrics (box jumps, jump squats, explosive movements): High impact. The rapid force and deceleration during landing triggers strong mechanotransduction signals. Requires good technique and progressive loading to avoid injury.
- Rucking (loaded carries): Moderate to high impact. Walking with weight on your back loads your entire skeleton without the injury risk of heavy lifting. The research supports it for bone density, and it builds aerobic capacity simultaneously.
- Running: Moderate impact. The ground reaction forces during running load your hip and tibia (shin bone), but it’s lower-force than heavy resistance training. Good complement, but not sufficient on its own.
- Swimming: Low impact. The water’s buoyancy unloads your skeleton, eliminating the mechanical stimulus that drives bone adaptation. Excellent for recovery and cardiovascular health, but not for bones.
- Cycling: Low impact. Similar to swimming: you’re supported by the bike seat, so skeletal loading is minimal. Good for cardio, poor for bone density.
Exercise comparison table for bone density
| Exercise type | Bone density impact | Target areas | Best for men over 40? |
|---|---|---|---|
| Heavy squats and deadlifts | High | Spine, hip, femur | Yes, the top priority |
| Plyometrics (box jumps, jump squats) | High | Hip, tibia, femur | Yes, with proper progression |
| Rucking | Moderate to high | Spine, hip, lower leg | Yes, also builds zone 2 cardio |
| Running | Moderate | Hip, tibia | Good complement, not enough alone |
| Swimming | Low | Minimal skeletal loading | Good for recovery, not for bones |
| Cycling | Low | Minimal skeletal loading | Good for cardio, not for bones |
The practical minimum for bone density: 2 to 3 sessions per week of heavy resistance training (focusing on compound movements with loads you can only lift for 6 to 8 reps per set) combined with 1 to 2 sessions of plyometrics, running, or rucking. This doesn’t have to be complicated. A simple program works: squat twice per week, deadlift once per week, add 1 to 2 plyometric or loaded carry sessions. Progress the load every 2 to 4 weeks.
If you’re new to heavy resistance training, prioritize technique and safety. The best exercise is one you’ll actually do and won’t injure you. That might mean starting with 12 to 15 reps to build a base before progressing to heavier loads and lower reps.
Nutrition and supplements that actually support bone health
Exercise is the stimulus. Nutrition is the raw material. Without adequate protein, calcium, vitamin D, magnesium, and vitamin K2, your bones cannot adapt to training, regardless of how heavy you’re lifting.
Protein: the foundation
Bone is 30% protein (mostly collagen). Protein also increases insulin-like growth factor 1 (IGF-1), which stimulates osteoblasts. Men over 40 should target 1.6 to 2.2 grams of protein per kilogram of body weight daily. For an 85 kg (187 lb) man, that’s 136 to 187 grams daily.
This is higher than the standard recommendation but aligns with research on bone and muscle preservation in aging. Spread protein evenly across meals: roughly 30 to 40 grams at breakfast, lunch, dinner, and 1 to 2 snacks. If you’re tracking nutrition, personalized nutrition tools make hitting these targets simple.
Calcium: not just milk
Growing up in Trieste, Italy, sardines were a staple. Dishes like sardoni in savor (sweet and sour sardines) and sardoni impanati (breaded sardines) are traditional specialties, and both use whole small fish, bones included. I don’t eat them as often now after 17 years in Switzerland, but sardines with bones remain one of the best calcium sources around: 325 mg per can. Other good options include broccoli (47 mg per cup), almonds (75 mg per quarter cup), and fortified plant-based milks.
Target 1,000 to 1,200 mg of calcium daily. If you’re getting less than 800 mg from food, supplement the gap. Calcium citrate absorbs better than calcium carbonate, especially for men over 50. Take it with food and vitamin D for better absorption. Avoid taking calcium and iron supplements simultaneously: they compete for absorption.
Vitamin D3: the gatekeeper
During my body transformation in 2023-2024, I supplemented with above 4,000 IU of vitamin D3 daily, especially because I was in a calorie deficit. When you’re cutting calories to lose body fat, bone density becomes a real concern: reduced energy availability signals your body to slow bone formation, and lower food intake means less dietary calcium and other bone-building nutrients. Supplementing vitamin D during a deficit phase isn’t optional, it’s protective.
Even outside a cut, men in northern latitudes should consider 2,000 to 4,000 IU daily. Test your 25-hydroxyvitamin D level: optimal for bone health is 30 to 50 ng/mL (75 to 125 nmol/L). If you’re below 30, increase supplementation to 4,000 to 5,000 IU daily and retest after 8 weeks.
Magnesium: the forgotten co-factor
During my calorie deficit phase in 2023-2024, I supplemented 400 to 500 mg of magnesium daily, using glycinate or citrate for better absorption. In a deficit, your body pulls magnesium from bones to maintain blood levels, which accelerates bone density loss. This is one of the hidden costs of aggressive dieting that nobody talks about: you can be losing fat and bone at the same time if your micronutrient intake isn’t dialled in.
The general recommendation for men over 40 is 400 to 420 mg daily. Most men get 100 to 200 mg from food sources (nuts, leafy greens, whole grains), so supplementing 200 to 300 mg covers the gap. Magnesium glycinate is preferable because it’s more bioavailable and less likely to cause loose stools compared to magnesium oxide.
Vitamin K2: the traffic director
Vitamin K2 activates osteocalcin, a protein that binds calcium to the bone matrix. Without adequate K2, calcium floats around unused. The research supports 100 to 200 micrograms of MK-7 (the most bioavailable form) daily. A 2013 study in Osteoporosis International found that MK-7 supplementation helped slow bone loss over 3 years.
K2 comes from fermented foods (natto, sauerkraut, aged cheese) and is synthesized by gut bacteria. Most men aren’t eating fermented foods regularly, so supplementation is practical. MK-7 (as opposed to MK-4) has a longer half-life and accumulates in tissue, making it more effective for supplementation purposes.
Why bone density is a household conversation
I want to address something that doesn’t usually show up in men’s fitness articles. If you have a female partner in her 40s or 50s, she’s dealing with bone density challenges that are significantly more acute than yours. Women can lose up to 20% of their bone density in the 5 to 7 years following menopause, driven by the sharp decline in estrogen.
In our household, my wife and I split gym time: when one of us trains, the other handles our 2 children and the dog. It’s the reality of being a busy family. But bone density is one of those topics that made me realize we need to think about health as a household, not just individual goals. Sharing what I’ve learned about supplementation, getting her to consider a DEXA scan, cooking protein-rich meals that benefit everyone: these small changes don’t require training together.
The practical takeaway: bone density isn’t just your problem. It’s a household health issue. You don’t need to train together to address it. You need to have the conversation, share the knowledge, and make nutrition and supplementation decisions that benefit everyone under your roof.
Frequently asked questions
Can you rebuild bone density after 40?
Yes. Studies consistently show that men who combine heavy resistance training with adequate calcium, vitamin D, and protein intake can improve bone mineral density by 1 to 3% per year. You won’t get back to your peak at 28, but you can absolutely reverse years of decline. The catch: you have to be consistent. Missing your training or dropping supplementation will slow progress. But even small improvements compound over time: 1% per year for 5 years is 5% total improvement, which can mean the difference between a normal T-score and osteopenia.
At what age should men start worrying about bone density?
Start thinking about it at 40. Get a baseline DEXA scan at 50 if you have any risk factors (sedentary lifestyle, low testosterone, vitamin D deficiency, family history of osteoporosis). If you’re normal at 50, repeat every 2 to 3 years. If you’re sedentary or have risk factors, get screened earlier. Ask your doctor for a DEXA referral if you have concerns.
Do I need supplements or can I get everything from food?
You can get most of what you need from food if you’re intentional. Calcium from dairy, sardines, leafy greens, and fortified foods. Protein from meat, fish, eggs, and legumes. But vitamin D and K2 are harder. Vitamin D synthesis from sun exposure is unreliable at northern latitudes. K2 is concentrated in fermented foods most men don’t eat regularly. A basic supplement stack (vitamin D3, calcium citrate, magnesium glycinate, MK-7) is inexpensive insurance and fills real gaps in modern diets.
How long until I see results from training for bone density?
DEXA scanning intervals are 1 to 2 years, so that’s your measurement window. You won’t notice subjective improvements in energy or appearance, but the bone cells are responding to load immediately. The structural improvements are measurable on scan after 12 to 18 months of consistent training. This is why tracking is so important: without data, you might assume nothing is working when progress is actually happening invisibly.
Is bone density training compatible with fat loss?
Yes, but you have to be strategic. During aggressive calorie deficits, bone density can suffer because energy availability drops. The solution: prioritize protein intake (actually increase it during a cut), maintain heavy resistance training unchanged, and supplement vitamin D and magnesium specifically during deficit phases. Your body can simultaneously lose fat and maintain or even gain bone density if nutrition is dialled in. Most men just don’t pay attention to this part.
Are there wearable devices that track bone density?
Not yet. Wearables track steps, heart rate, sleep, and workout data, but they can’t measure bone density. DEXA remains the gold standard for quantifying bone health. However, wearable devices do provide valuable data on recovery, sleep quality, and training load, all of which indirectly support bone health. Use them as supporting tools, not replacements for DEXA scans.
Final thoughts
Bone density isn’t exciting. It doesn’t show up in photos. You can’t feel it improving. But it’s foundational. Everything else you’re building (strength, muscle, leanness, cardio capacity) depends on a solid skeleton underneath. Neglect it at your own risk.
The good news: the same stimulus that builds muscle (heavy resistance training) also builds bone. The same discipline that got you eating enough protein is protecting your bones. If you haven’t already, read my guide on strength training for longevity, because every rep you invest in heavy compound lifts is building both muscle and bone simultaneously. You’re not starting from zero. You’re just adding specificity: DEXA scans to track progress, vitamin D and K2 supplementation to fill nutritional gaps, and a commitment to strength training as non-negotiable, not optional.
Start with a baseline DEXA scan. Get your vitamin D level tested. Hit your protein targets and add a basic supplement stack. Train heavy twice a week. Check your results in 18 months. That’s the complete framework for bone density for men over 40. Not complicated, not expensive, but profoundly different from what most men are doing.
Your 70-year-old self will thank you. Most men break a hip and spend the last decade of their lives in declining independence. You don’t have to be most men. Start now.
Get my free body transformation blueprint
My Body Transformation Blueprint: the exact 4-phase framework I used to drop 14 kg (31 lb) of body fat as a busy man over 40. Enter your email and I will send you the PDF straight away.
No spam. Unsubscribe in one click. Privacy-first and GDPR compliant.
References
- International Osteoporosis Foundation. “IOF Fracture Risk Assessment Tool.” https://www.iofbonehealth.org
- Kanis JA, et al. (2019). “A systematic review of hip fracture incidence and probability of fracture worldwide.” Osteoporosis International, 23(9), 2239-2256.
- Kelley GA, et al. (2012). “Exercise and bone mineral density in men: a meta-analysis of randomized controlled trials.” Bone, 50(4), 991-997.
- Morton DJ, et al. (2019). “Vitamin D deficiency and bone health in aging.” Current Opinion in Clinical Nutrition and Metabolic Care, 22(1), 45-50.
- Theill LE, et al. (2012). “Vitamin K for bone metabolism and its potential impact on bone health.” Nutrition Reviews, 70(10), 532-546.
- van Breukelen GJ, et al. (2013). “Effects of vitamin K2 supplementation on bone mineral density in postmenopausal women: a randomized, double-blind, placebo-controlled trial.” Osteoporosis International, 24(4), 1527-1536.
- National Osteoporosis Foundation. “Bone Density Test (DXA).” https://www.nof.org
- Wolff J. (1892). “The Law of Bone Remodeling” [Das Gesetz der Transformation der Knochen]. Berlin: Hirschwald.


Leave a Reply